Happy 70th Anniversary Defibrillation!
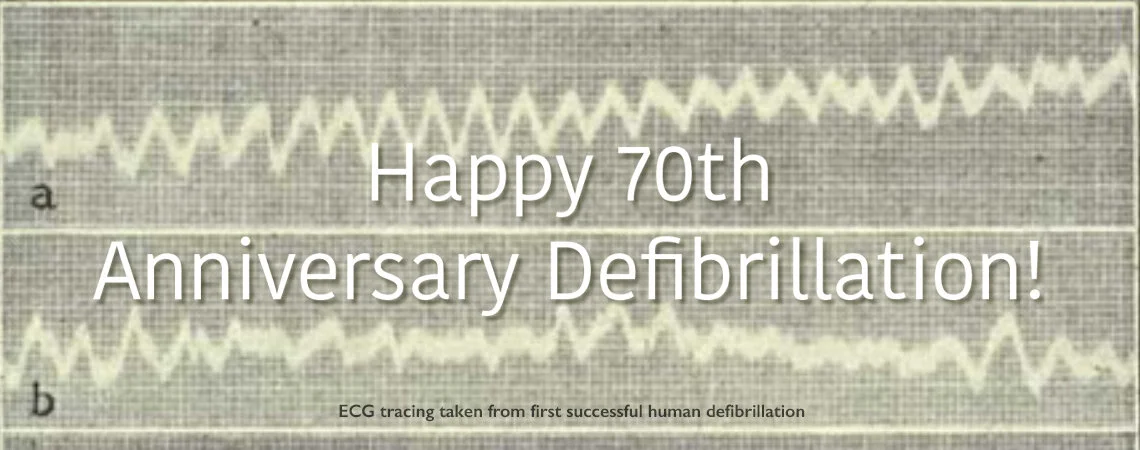
The first successful human defibrillation occurred 70 years ago in 1947. Much has happened since that milestone.
The event occurred in the operating room of University Hospital. The patient, a 14-year-old boy, was undergoing an operation for a funnel chest deformity and during closure of the chest the pulse suddenly ceased. Dr. Beck reopened the chest, saw the fibrillating heart, and started open chest massage while calling for the experimental defibrillator to be brought from his laboratory. He continued massage for 45 minutes until the device was rolled in. After two AC shocks the boy’s heart began contracting normally. (JAMA, 135:985-986, 1947) Several days later he was discharged.
Scientific Progress
From this seminal event, the science of defibrillation evolved, first to closed chest defibrillation, then DC defibrillation, finally to battery-operated devices. The therapy spread from operating rooms to coronary care units and emergency departments and in the late 1960s left the hospital and started appearing on mobile intensive care units. The first portable EMS defibrillators (used by paramedics) emerged in the early 1970s. In 1980 the automatic implantable cardioverter-defibrillator was invented. Automated external defibrillators began appearing in the late 1980s allowing the therapy to be delivered by EMTs and lay people.
During this 7 decade spread considerable science has helped define optimal waveforms (bi-phasic) and energy (lower than originally used). Automatic external defibrillators have become smaller, more sophisticated, and less expensive. It is unequivocally clear (and has been since the days of Beck) that the sooner the defibrillatory shock is provided the better the outcome.
While the science and technology of defibrillation have advanced the ability to rapidly provide defibrillation has not improved much over this time. The fundamental problem in treating ventricular fibrillation is the time interval from the event to EMS arrival. Though widespread CPR training and telephone-CPR have helped to extend the window of opportunity in which a defibrillator may be effective, there is only so much an EMS system can do to achieve rapid defibrillation. (To be fair, AEDs and public access defibrillation have helped to a small degree.)
The Need for a Game Changer
We need a disruptive technology to allow defibrillation to become a consumer device. Researchers and physicians have argued for such a device. Today, using off the shelf components (with a cost far less than today’s AEDs), it is possible to make a consumer device capable of a few shocks, intended for single use powered by AA batteries, and then disposed. Shelf life can be 10 years. However there is a giant gap between possible and actual with many regulatory, safety, and reliability issues. And yet similar issues were raised against oximeters, glucometers, epipens, and other “dangerous” technologies in the hands of consumers. Think of the analogy with CPR. CPR started as an operating room procedure then spread to the hospital and then to EMS personnel and finally to the public. Similarly defibrillation started as an operating room procedure spread through out hospitals, then to EMS (initially to paramedics and then to EMTs), and finally to public locations. Why shouldn’t the final step be directly into people’s homes? Something to think about.
The Resuscitation Academy







There are opportunities to significantly increase survival from out of hospital cardiac arrest. Implementation of existing standards and training programs for telephone CPR and high-performance CPR will do much to improve survival.